History submitted by Dr Abhishek Jain, INTERN at PCMS & R.C. ,Bhopal
A male patient aged 50 years was admitted to our Hospital in autumn 2013 with Chief complaints of Chest pain which was Severe in intensity, diffusely located on the LEFT side of chest, associated with a feeling of heaviness over that region.
Chest pain was also associated with PROFUSE SWEATING and pain occurred in patient while performing his daily routine activities.Initially pain subsided in terms of Intensity on its Own, after 10 mins of its onset and further decreased upon intake of a medication ,taken Sub-lingually.
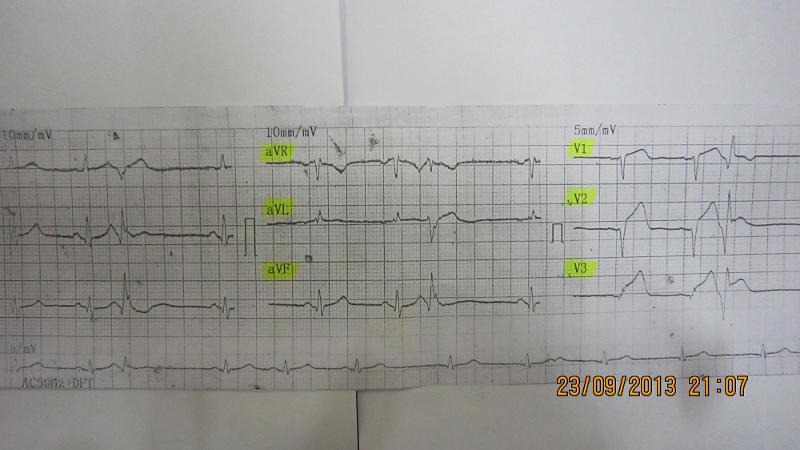
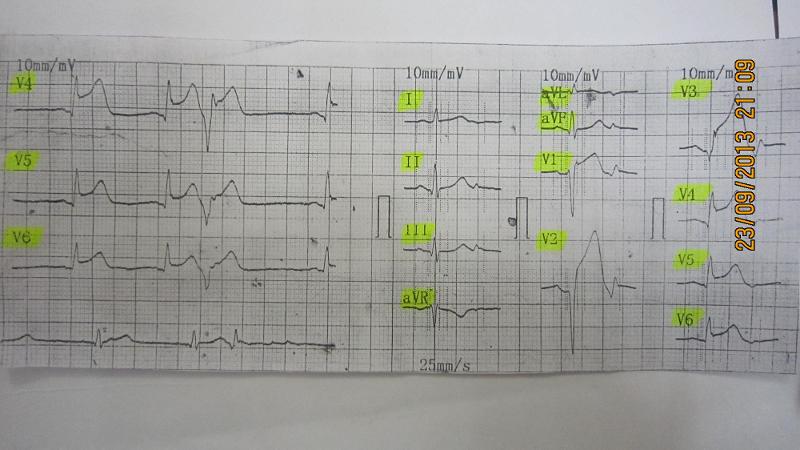
Patient was admitted to our hospital after 8 to 9 hours of first episode of Chest pain and sweating, though ECG was done within 1 hour of this episode nearby his home at a clinic (see attached ECG after one hour...the dates on the ECG are that of the scanner and not the actual date the ECG was taken...).
The patient had 50% reduction of his chest pain and repeat ECG showed further appearance of q waves not just in V1 and V2 as in the ECG after one hour but also in V3.V4,V5. ST elevation was persistent and >5mm in all leads.
OTHER significant History- Patient has an addiction to tobacco for past 20 years.
Examination of Patient-
Day 1 of admission:
- Pulse- 70/min, BP-110/80 mm of Hg , RR-18/min, Temp - afebrile .
- Clubbing,Pallor, Edema , Cyanosis, Tremors - absent
- RS: B/L chest - CLEAR, no added sound; CVS: S1, S2 audible ; P/A system- soft,non tender, Spleen & Liver not palpable ;CNS :Pt is conscious,oriented and no Focal defect seen, patient could easily narrate his History.
Investigations done-
On Day 1 of admission-
1)CBP:-
Parameter: Result: Ref. Range Opinion
-WBC: 9.3 x 10^9/L 4 to 10.0 within normal range
-DLC: P- 76%, L-21%, M-1%, E-2%
-Hb: 12.5 g/dl 11- 16.0 within normal range
-RBC: 4.11 X 10^12/L 3.50-5.50 within normal range
-PLT: 206 x 10^9/L 100-300 within normal range
2)RANDOM BLOOD SUGAR: 113.O mg% <140mg% within normal range
3)Renal function test:
-Blood Urea 27.8mg% 10 - 40mg% within normal range
-S. Creatinine 1.0mg% 0.7 - 1.4mg% within normal range
On Day 2 of admission-
1)Lipid Profile:
Serum -Cholesterol: 207.0 150-250mg% within normal range
-HDL: 50.0 >35mg% within normal range
-LDL: 143.0 <150mg% near upper limit
-VLDL: 14.0 upto 30mg% within normal range
-TG: 70.0 upto 150mg% within normal range
RISK FACTOR: 4.1 4.4 - 11 slighly below lower limit
2)Urine-routine & microscopy: PUS CELL "OCCASIONALLY" found/hpf
3)CPK- MB,Serum 327 <24 U/L Highly Raised
(sample collected on day 2)
On Day 3 of admission-
-ECHOCARDIOGRAPHY( report enclosed) :
Impression: CORONARY ARTERY DISEASE - LAD(Left Artery Descending) Akinetic LAD territory with mild Left Ventricular Dysfunction
Treatment given after admission:
Antiplatelets (Tab Clopitab 75mg , Tab Dispirin), Beta Blockers (Tab Met XL 25 mg od), Analgesics (Tab Sorbitrate, Inj Fortwin 1amp stat and sos) and antocoagulant Inj LMWH 6 ml.
Now the question is should we offer thrombolytics to STEMI patients with well developed 'q' waves who have arrived in casualty within 9 hours with 50% reduction in chest pain? Do thrombolytics have benefits in terms of patient related outcomes in such situations? Any papers throwing further light on this will be appreciated.
Few papers searched and shared here by Dr Abhishek:US National Library of Medicine , National Institutes of Health
Related Link-
Patient's perspective: History
uploaded by Miss Anamika Sharma, PCMS Medicine, Research Lab, Bhopal, Fall 2013
Patient Particulars - Age-49 year, height - 5.5,weight - 63,sex
- male
History of Illness - 12 sep.2013 ko mujhe 1st time
heart attack aaya,jab mujhe attack aaya to me so raha the.almost time morning
ke 4 baje huye the.
meri nind seene me dard ki wajah se khul gai.4 baje mene dubara sone ki koshish
ki bat mujhe nind nahi aai.pehle mujhe seene ke bich me dard ho raha the uske
baad mujhe dhere - dhere seene ke aas - pass bhi dard hone laga or hantho me
khichav hone laga.ager me apne hantho ko free rakhta hu to mera dard badta hi
ja raha the.or hantho ko bandh kar rakhu to dard ko thoda aaram mil raha the.
morning 4 baje se 8 baje tak dard kam nahi hua.or badta gaya.mene fir pass ke
local doter ko dikhaya to usne ecg ki.
or july 2013 se me barish me geela ho gaya the.to mujhe thand lag kar fever
aaya the.uske baad se mujhe fever har kabhi aa jata the.oe mera muh bhi bahut kadwa rehta the. or mere pero ke talwe
or hantho ki gaddiyo par all time garmahat bani rehti.or mera khana bhi bahut
kam ho gaya july se.totaly mene se khana july se teek se khaya hi nahi.meri
bhukha bhi kam ho gai. es wajah se weakness bahut aa gai hai.mujhe sochna padta
h ki me ager chaluga to gir na jau.aankho me dundhalapan aata hai,or kabhi kabhi
gas problum bhi hoti hai.