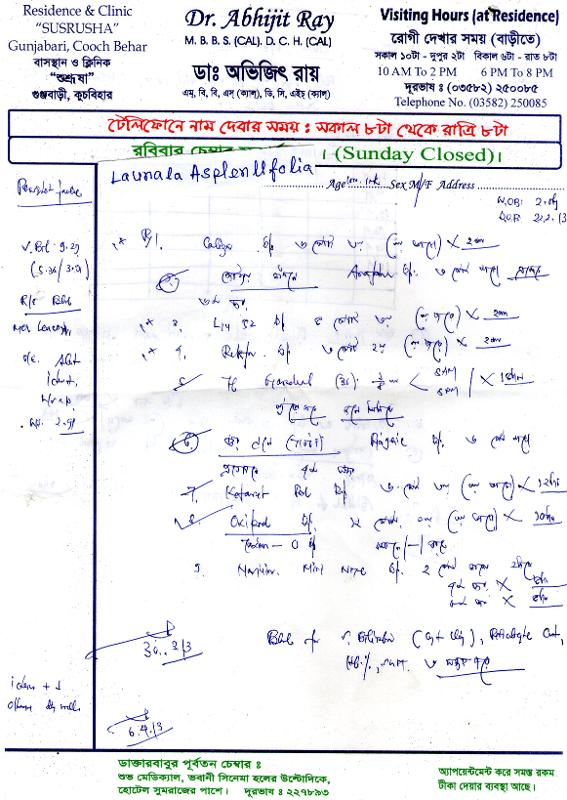
49 day old child noted to have jaundice since the last 3 weeks.

Initial Outputs from UDHC team:
From: Rakesh Biswas
Sent: Sat, 13 Apr 2013 14:37:30
Eye examination should include - e/o cataract, chorioretinitis,
CMV IgM is essential
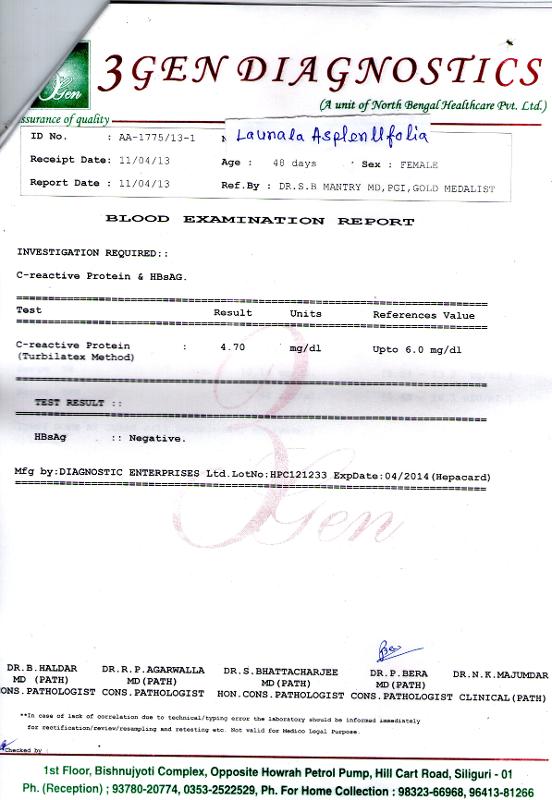
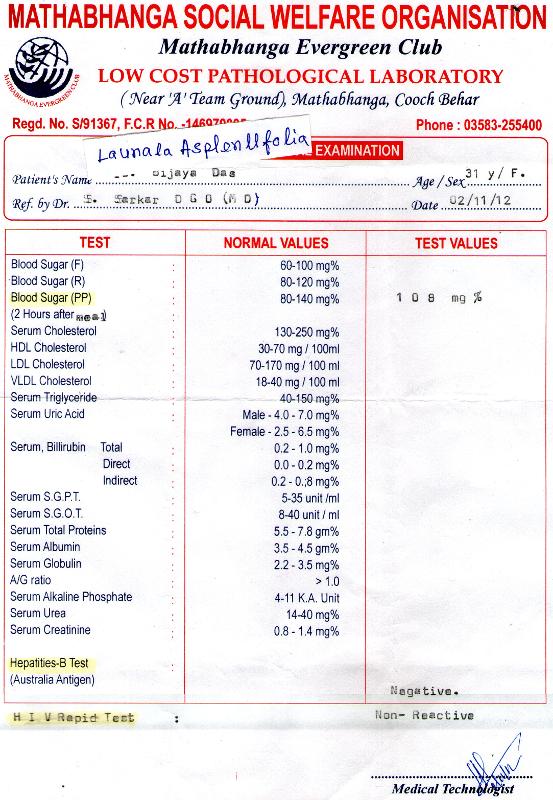
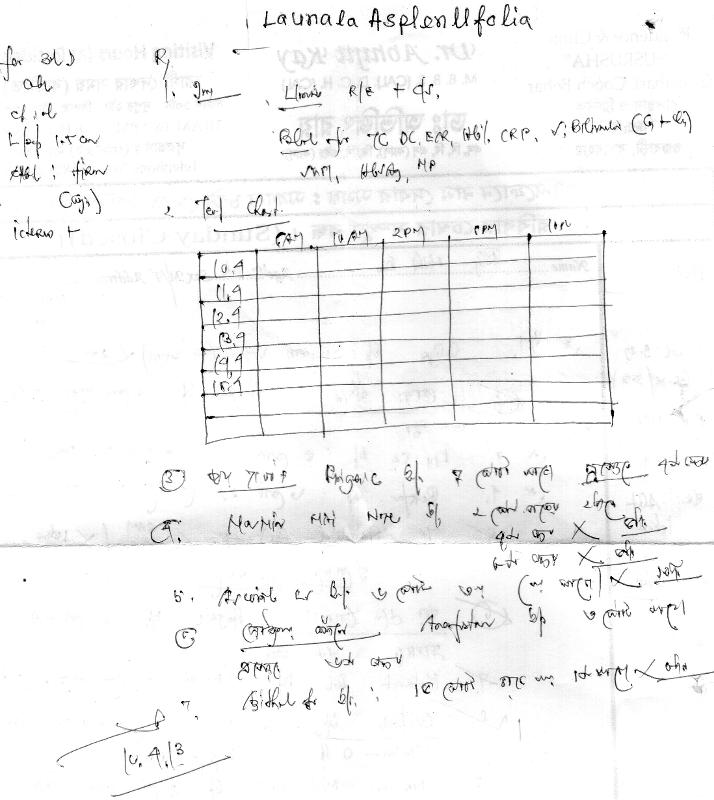
LFT- serum albumin and serum gamma glutamyl transferase are important.
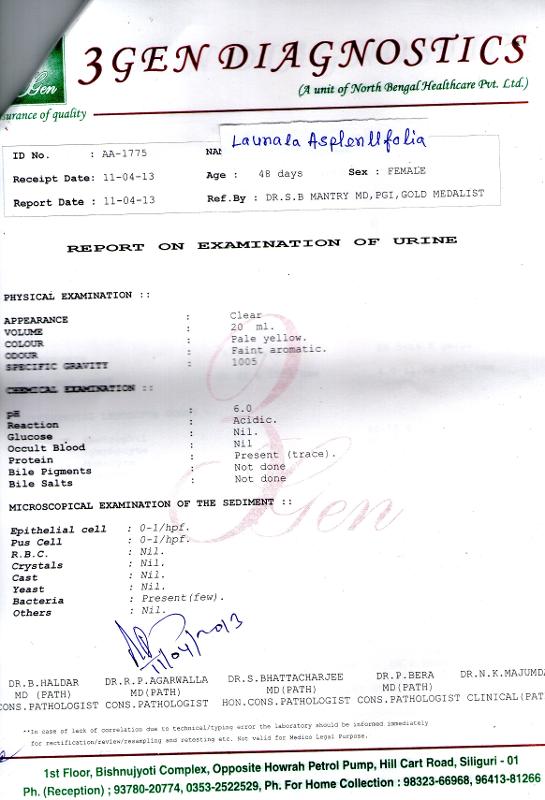
Benedict's test for reducing substance in urine should be done after
pretreatment of urine with conc. Hydrochloric acid to be able to
detect lactose.
Questions to the parent and Local Physician:
Regarding the baby's appearance, does she resemble any of her parents
or other relatives? Is her facial appearance- abnormal?
Is the baby feeding poorly now?
If yes, since when?
Is it after starting Gardenal? Is the baby still on Gardenal? If yes,
how many ml in a day?
Is the poor activity only during fever and cold episodes?
How many times does the baby pass urine in 24 hours?
It would be useful to document the weight weekly on follow up.
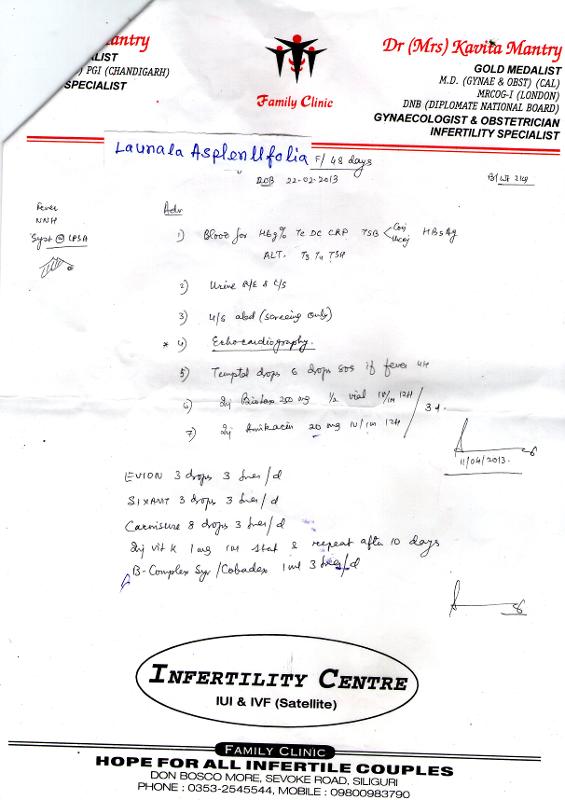
Has she been prescribed vitamin A & vit D? (it is not clear from the
prescriptions)
It is important to give her weekly vitamin K injections
regards,
Rakesh Biswas for the ArogyaUDHC team
From: Rakesh Biswas
Date: Fri, Apr 12, 2013 at 10:50 PM>
For patient input
http://care.udhc.co.in/INPUT/displayIssueGraphically.jsp?topic_id=273
Local daktarer jonye suggestion:
Aro kichu test
Chest X ray
Complete LFT including AST/ALT and serum albumin
Urine for reducing substances
From: Shruti Sarkar
Date: Fri, 12 Apr 2013 21:33:06 +0530
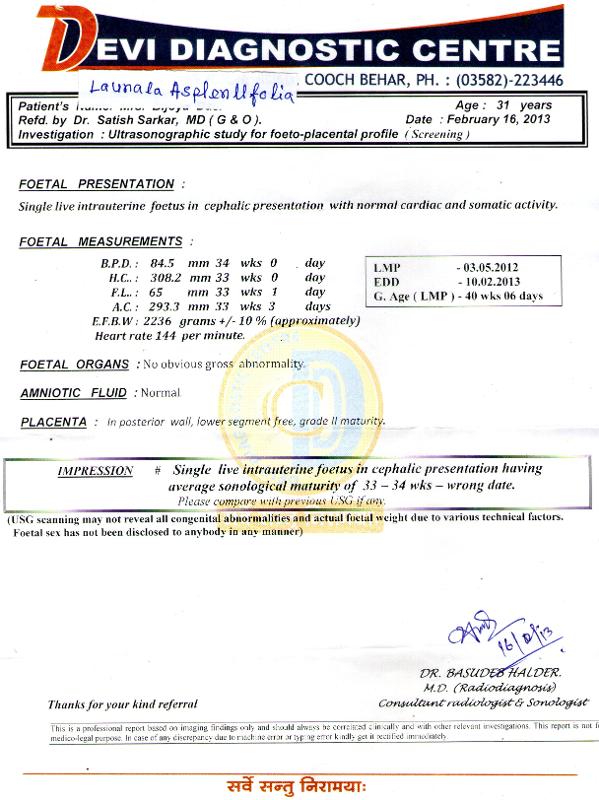
What I understood was that this is a 6 weeks old baby born at term and low
birth weight, had some feeding difficulties and has persistent
jaundice
that is direct.
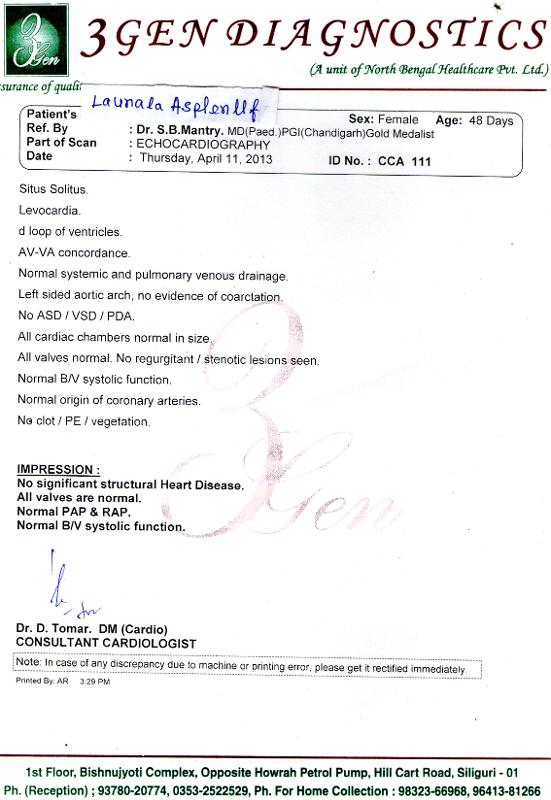
The important causes to consider are intrauterine infections, i.e. Rubella
and CMV mainly, billiary atresias, intra or extrahepatic as gall bladder
visualised extrahepatic unlikely and also to rule out galactosemia. Out of
all the causes high possibility of CMV
Needs a complete physical examination, eye examination, urine for reducing
substance and further imaging of liver if indicated. Further prognosis
depends on the cause
Shruti Sarkar
Associate Professor,
PCMS, Bhopal
Tabula rasa processing:
Last week of May 2013 update:
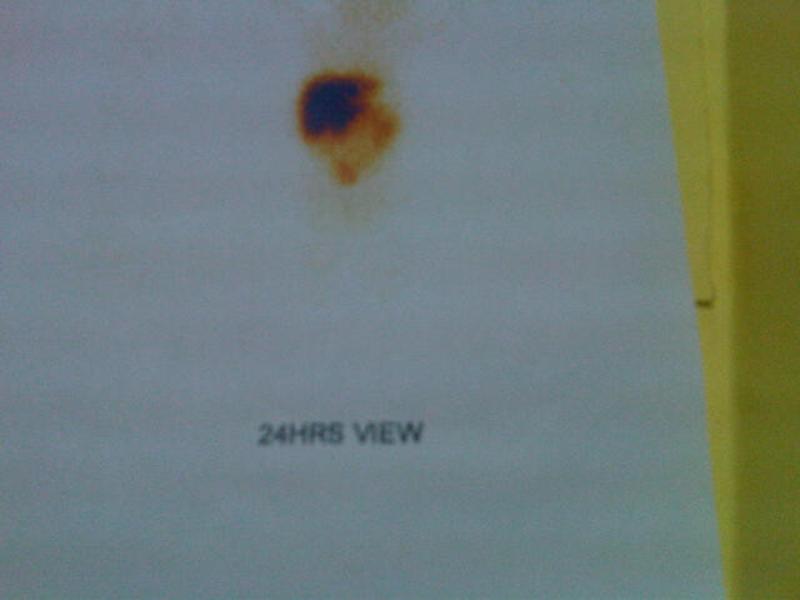
The patient was reviewed in PCMS Bhopal and further work up including a HIDA scan (figure uploaded to input page) and other viral markers made us conclude that it was a neonatal hepatitis and hopeful that it would recover spontaneously. A liver biopsy may have revealed giant cell hepatitis but it was decided not to go ahead with this invasive procedure. A follow up on the liver size would remain of utmost importance and we may be able to depend on our social worker Mr Kar to send us a monthly update on the baby's liver span (the measurement of which can be taught through informational support).
May 2014 update:
Slight anorexia since last 2 weeks. LFT shows mild rise in AST (0.5 times with normal ALT) and mild rise of Alkaline phosphatase (0.2 times) with a total bilirubin of 1.68 and direct 0.93 mg%).